I teach an advanced EBM co-enrolled elective in the Spring semester to 3rd and 4th-year medical students.Below is a screen shot of the course home page.
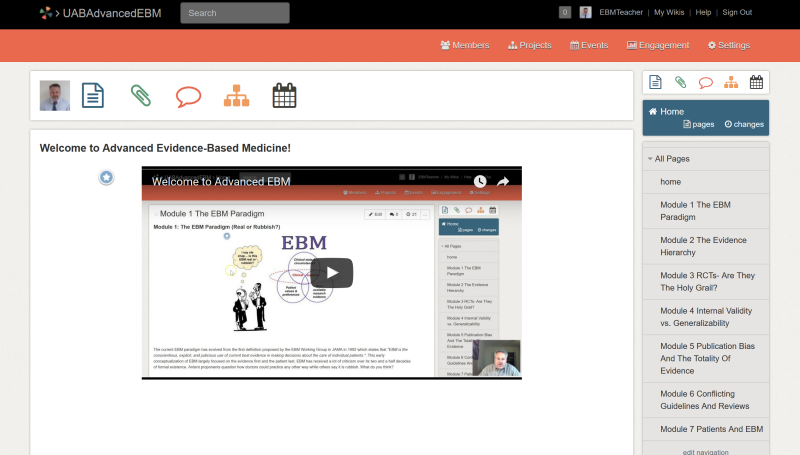
This year I decided to revamp it completely and make it more philosophical. It was a challenge to decide what topics to include. You can see the topics I plan to cover along the right side of the image. I wanted them to be thought provoking and also useful at some level and not something taught in the usual EBM course. I also made some other big changes after being inspired by 2 classes (Introduction to Openness and Social Network Learning) I recently took as part of my Master of Educational Technology degree (Thanks Fred Baker and Jackie Gerstein). Here are the changes:
- It’s open (all materials are free to use and anyone can take the course at any time). I hope to get some non-UAB students to take the course at the same time as my UAB students- a mini-MOOC so to speak.
- Students will use social network tools extensively to enhance learning.
- Students get a say in what they learn. I have designed the learning modules but I encourage students to develop their own learning module to replace one of the ones I developed.
- Students will learn the value of social media for finding, creating, and sharing information.
- Students will learn about personal learning networks and how to cultivate them.
- Students will be exposed to learning activities they probably haven’t been exposed to in the past or used very much (e.g. jigsaw activity, curation, concept mapping, blogging, tweeting) in medical education.
I hope these changes will enhance the ability of students to make meaning of this material. If nothing else I enjoyed creating a new class.