In this installation I want to jump ahead in Greenhalgh’s paper to address her last cause of the EBM crisis: “Poor fit for multimorbidity“. Not to worry, I will come back in a future post to cover the remaining “problems” of EBM.
I concur with Greenhalgh that individual studies have limited applicability by themselves in a vacuum to patients with multimorbidity. Guidelines don’t help a they also tend to be single disease focused and developed by single disease -ologists. So is EBM at fault here again? Of course not. EBM skills to the rescue.
The current model of EBM demonstrated below contains 2 important elements: clinical state and circumstances and clinical experience.
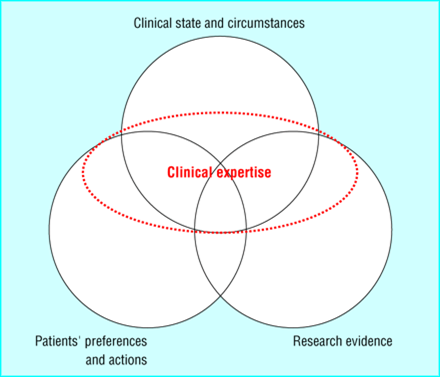
Clinical state and circumstances largely refers to the patient’s comorbidities, various other treatments they are receiving, and the clinical setting in which the patient is being seen. Thus, the EBM paradigm is specifically designed to deal with multimorbidity. Clinical expertise is used to discern what impact other comorbidities have on the current clinical question under consideration. and, along with the clinical state/circumstance, helps us decide how to apply a narrowly focused study or guideline in a multimorbid patient. Is this ideal? No. It would be nice if we had studies that included patients with multiple common diseases but we have to treat patients with the best available evidence that we have.

so your strategy here and in the previous posts seems to be mostly to deny that the problems she points out, which you acknowledge to be real, involve any indictment of EBM, because EBM is clinical expertise skillfully applied, which would exclude the kind of problems she alludes to.
it seems to me a bit of a cop out to use EBM as a synonym for “clinical judgment”; isnt that kind of what you’re doing here? Clinical judgment (or expertise) is the judicious selection and assessment of multiple possible kinds of evidence that might bear upon a decision and then making the decision properly, right? would anyone in the pre-EBM era have disagreed with such a characterization? and if you’re now going to call that “EBM”, havent you just effectively denied that EBM is anything new or distinctive?
I dont deny the problems exist but I dont blame them on EBM principles. The current EBM paradigm is the combination of patient values/expectations, clinical state and circumstances of the patient, the best available research evidence and clinical experience. I dont call it EBM. Its a paradigm developed over the last decade or so since the term EBM was coined. I think what is new is that medicine was more paternalistic in the past. Patient values were not viewed as primal like they are in the current EBM paradigm. Clinical judgment is important. The evidence and patients tell us what we could do but our judgment guides us to what we should do. EBM skills have also helped us understand where you can be misled by evidence and how to use the evidence. That is also new.
perhaps the way we talk about patient preferences has indeed changed. im not sure the present way of talking about them is at all accurate. i do not believe that “patient preferences” (without qualification) are really at all a kind of equal partner in the interplay between research evidence, pathophysiological rationale, and clinical experience as we make clinical decisions. what we really acknowledge are a subset of patient preferences, those that involve negative determinations about our suggestions; and positive preferences only insofar as these are compatible with medical norms and standards. That a patient wants an mri when that is not indicated is a patient preference that cuts no ice in our clinical judgments. nor do i honor patient preferences for e.g. addictive substances (although i may acknowledge such preferences and try to change them or work around them).
maybe some formal recognition of patient preferences is indeed a new element in our notion of what constitutes good clinical judgment. that seems to me rather weak tea if it is posited as what makes “ebm” a new paradigm.
it makes more sense to me to think of “ebm” not as clinical judgment or expertise as per the area of overlap on your diagram but instead as the complex of skills involved in assessing clinical research and bringing that research to bear on clinical decisions. That is, it is one element in the complex of abilities that makes up clinical judgment, not clinical judgment itself. And Greenhalgh et al are correct, it seems to me, to suggest that the importance of these skills has perhaps been overblown at times by EBM enthusiasts.