Composite endpoints are commonly used in studies. A composite endpoint is an endpoint composed of several other endpoints. If a patient experiences any one of them they are considered to have experienced the endpoint of the trial. For example, a composite endpoint in a typical cardiovascular study includes nonfatal MI, nonfatal stroke and cardiovascular death. A patient doesn’t have to have all three just one of them.
Why use composite endpoints? The main reason is to reduce the number of patients needed in the study. The chance of a patient having any one outcome is much less than having any one of three outcomes. They are also used to potentially reduce the length of follow-up needed in a study. A patient is likely to develop one of three outcomes more quickly than any one outcome or one of the components of the composite can occur sooner than another (e.g. doubling of serum creatinine vs. initiation of hemodialysis).
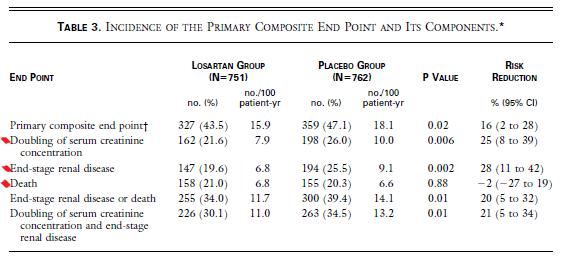
Not all composites are created equal. Some are good and many are poorly developed. Examine the composite outcome below from the RENAAL trial published in the NEJM in 2001. The primary efficacy measure was the time to the first event of the composite end point of a doubling of the serum creatinine concentration, end-stage renal disease, or death. What do you think? Is this a good composite or a poor composite? (Note: I put a red mark next to the components of the composite)
From the RENAAL trial, NEJM 2001
I think this is a poorly designed composite. Why do I say that? A good composite should have the following characteristics:
- Each component should be valued equally by patients,
- Each component should occur with similar frequency, and
- The intervention should have the same relative effect on each component.
With this in mind, reevaluate the RENAAL composite endpoint. Hopefully you agree with me that its not a good composite endpoint. Let’s examine it more closely.
Issue #1: would patients consider each of the components to be of equal value? Patients would not consider death and doubling of serum creatinine as being equal. Clearly they would value death as a much worse outcome. So this composite fails here.
Issue #2: do each of the components of the composite occur with equal frequency? Looking at the percentages of the components in the losartan group they are pretty close to each other (21.6%, 19.6%, and 21%) so I would give the composite a pass on this criterion.
Issue #3: does the intervention (losartan) have an equal effect on each of the components of the composite? Look under the risk reduction column and the answer is no. Doubling of serum creatinine is reduced by 25% and end stage renal disease by 28% but death is actually increased by 2%. Thus, the composite fails on this criterion.
What should you do if the composite endpoint is a bad composite? Just ignore the composite and look at the individual components. Even if a composite is a good one you should always examine the individual components. So in this case losartan reduces the risk of ESRD and doubling of serum creatinine but has no effect on mortality.
